What is the Rotator cuff?The shoulder joint is the articulation between the shoulder socket (part of the shoulder blade) and ball (the top of the arm bone). The Rotator cuff muscles originate from the shoulder blade, pass between the top of the arm bone (shoulder ball) and the top shelf of the shoulder blade bone (acromion) and insert through their tendons into the top of the arm bone around the shoulder joint ball. There are four such muscles and collectively, they are called rotator cuff muscles. The function of these muscles is to stabilise the shoulder ball into the socket while the big muscle on the outer aspect of the shoulder (deltoid) elevates the arm.
What is Impingement?
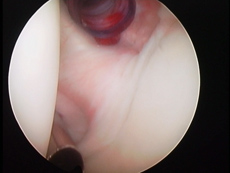
Rotator cuff tendons normally slide smoothly under the acromion (top shelf of shoulder blade bone) as the shoulder moves to lift or rotate the arm. Impingement happens when the rotator cuff tendons start to rub against the acromion as the shoulder moves. This rubbing causes an inflammation in the tendons, called tendonitis. The tendon of the supraspinatus muscle (one of the rotator cuff muscles) is the tendon normally affected by this process. Supraspinatus tendonitis is the most common cause of shoulder pain.
What causes Impingement?
As people grow older, the structure of the rotator cuff tendons weakens (a process called degeneration). This weakness means the tendons are unable to stabilise the shoulder ball, as the deltoid muscle elevates the arm. This means that as the arm is elevated, the shoulder ball rises and traps the rotator cuff tendons under the top shelf on shoulder blade bone (acromion). As the arm is elevated to chest height, the trapped tendon starts to rub against the acromion.
What does Impingement feel like?
People with impingement suffer mainly with pain due to the tendon inflammation (tendonitis). This pain is felt over the outer aspect of the upper arm, but occasionally radiates down to the elbow or back to the shoulder blade. The pain is aggravated by lifting the arm above shoulder height, putting the arm behind the back or lifting objects away from your body. In time some of these actions may become impossible and the shoulder feels stiff.
What can I do to make my Impingement better?
As the pain of impingement is caused by tendon inflammation (tendonitis), avoiding the activities that cause the pain is the best way of allowing the tendons to rest and the inflammation to settle. Anti-inflammatory medication may be helpful, but normally will not help without stopping the painful activities. If the pain does not settle within 6 weeks with these measures or restarts when you resume activities, you need to seek medical advice.
How can I find out if I have impingement?
Your doctor will examine you and if he or she suspects that impingement is the problem, this can be confirmed by an injection of local anaesthetic in the space between the rotator cuff tendons and the top shelf of shoulder blade bone (acromion). This is called a subacromial injection. If the pain is relieved by this injection, the diagnosis is confirmed. If there is doubt or the injection is not helpful, an Ultrasound scan or an MRI scan would help.
What happens if the Impingement continues without treatment?
As the process of impingement progresses and the structure of the tendons of the rotator cuff weaken further, the rotator cuff tendons finally tear. This process initially involves part of the thickness of the tendon (partial tear), then the full thickness of one tendon (complete tear) and gradually progresses to involve all four tendons of the rotator cuff (massive tear). Unfortunately, these tendons are unable to repair themselves.
How can Impingement be treated?
The initial aim of the treatment is to relief pain. The most effective way of doing that is an injection in the subacromial space (between the tendon and acromion) of a steroid. Steroids relief the tendon inflammation and reduce the pain within a few days. Once the pain is relieved, physiotherapy can be started to strengthen the rotator cuff muscles and allow better control of the shoulder joint as it moves.
If the pain is not severe initially, physiotherapy may be helpful without an injection. However, if the pain is severe, physiotherapy without an injection will aggravate the pain.
Unfortunately, the process of tendon degeneration, which initiates the problem, is a natural process and at the moment is not reversible.
 If physiotherapy is not helpful, can anything else be done?
If physiotherapy is not helpful, can anything else be done?
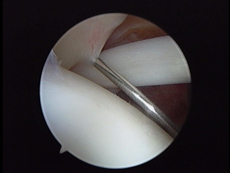
If the pain returns following a period of relief from the injection and physiotherapy, the only other option for treatment is surgery. This keyhole surgery removes the small part of the top shelf of shoulder blade bone (acromion) that is rubbing against the tendons, and is sometimes called acromioplasty or subacromial decompression. This will relief the pain in over 90% of people.
 This operation is done through two or three, 0.5 cm puncture wounds under a general anaesthetic. Most people would go home the same day and wear a sling for a few days until the shoulder is comfortable. The pain of the operation settles in 2-3 weeks and the original pain settles over a period of 3 months as the inflammation in the tendons settles. All pain free activities are allowed once the sling comes off. Any painful activity is to be avoided until the pain related to that activity settles. In general, anything you could do just before the operation, you can do within 2-3 weeks after the operation and all normal activities will be possible between 3 & 6 months after surgery.
This operation is done through two or three, 0.5 cm puncture wounds under a general anaesthetic. Most people would go home the same day and wear a sling for a few days until the shoulder is comfortable. The pain of the operation settles in 2-3 weeks and the original pain settles over a period of 3 months as the inflammation in the tendons settles. All pain free activities are allowed once the sling comes off. Any painful activity is to be avoided until the pain related to that activity settles. In general, anything you could do just before the operation, you can do within 2-3 weeks after the operation and all normal activities will be possible between 3 & 6 months after surgery.
What is a Rotator cuff tendon tear?
As mentioned above, the rotator cuff muscles attach themselves to the top of the arm bone with tendons. These tendons may tear as a result of a combination of two processes. Initially, this starts with weakening of the structure of the tendon (degeneration), as people get older. This leads to Impingement as explained above. The combination of Impingement and progression of the tendon degeneration eventually leads to a partial then complete tear of the tendon.
What does a rotator cuff tear fell like?
A tear in the rotator cuff tendons normally occurs without an injury in people in their late forties or over. This can, however, occur after an injury in younger or older people. People with a rotator cuff tendon tear have pain at night and during the day particularly with activities that involve stretching out forwards while lifting or activities involving twisting the hand behind their back. As the tear in the tendons becomes bigger, weakness and stiffness develop.
How can I find out if I have a Rotator cuff tendon tear?
Although your doctor or physiotherapist can normally diagnose these tendon tears as they get bigger, a small tear causing no weakness may be difficult to diagnose. Your doctor will, therefore, tend to organise for you to have an MRI (magnetic resonance) or Ultrasound scan to detect the tendon tear, assess the number of tendons affected and the size of the tear.
What treatments are available for a Rotator cuff tendon tear?
The options available to treat shoulder conditions normally revolve around steroid injections, physiotherapy and surgery.
i- Injection,
Steroid injections reduce the inflammatory reaction around the cuff tendons and as such relief the pain. However, the pain relief is frequently temporary. Repeated steroid injections weaken the tendon structure further.
ii- Physiotherapy,
Physiotherapy for rotator cuff tendon tears can provide some pain relief and strengthen the remaining rotator cuff muscles to try and compensate for the torn tendons. Obviously, this is beneficial and for people who are unfit for or are unwilling to undergo surgery is the mainstay of treatment. Also, in some situations when the tears in the tendons have become too large, surgery to repair the tendons is not possible and physiotherapy is the only option available.
 iii- Surgery,
iii- Surgery,
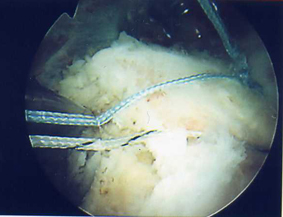
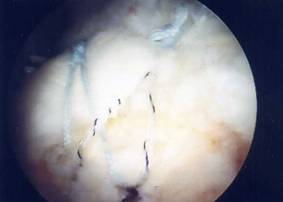
Surgery for rotator cuff tendon tears involves repairing the torn margin of the tendon to the area of the top of the arm bone where it originally inserted. This is done by inserting sutures into the tendons and into the bone of the top of the arm bone or using anchors to suture the tendons to bone. This operation is normally associated with removal of part of the top shelf of shoulder blade bone (called subacromial decompression or acromioplasty) to reverse the process of impingement of the tendons against that part of the bone. Traditionally, this surgery is done through an incision over the top and the front of the shoulder. In the Birmingham Knee & shoulder Clinic, this surgery is almost always performed as an arthroscopic (keyhole) operation.
Apart from the obvious advantage of keyhole surgery of a better cosmetic appearance, keyhole surgery has several advantages over open surgery. Keyhole surgery does not violate the deltoid muscle necessary for access with open surgery, involves less post-operative pain and shorter stay in hospital.
 Keyhole surgery to repair rotator cuff tendons is done through several 0.5 cm puncture wounds around the shoulder under a general anaesthetic. It involves a hospital stay of 1 night. A sling is worn for 3 weeks, but occasionally up to 6 weeks for larger tears. Pain tends to settle following surgery over a period of 3 months and function continues to improve for 1 year. Driving is not possible for 6 to 8 weeks after surgery. Return to work depends on the type of work and whether driving is necessary. Swimming is encouraged once the sling is of. Overhead and Contact sports are to be avoided for 4 months.
Keyhole surgery to repair rotator cuff tendons is done through several 0.5 cm puncture wounds around the shoulder under a general anaesthetic. It involves a hospital stay of 1 night. A sling is worn for 3 weeks, but occasionally up to 6 weeks for larger tears. Pain tends to settle following surgery over a period of 3 months and function continues to improve for 1 year. Driving is not possible for 6 to 8 weeks after surgery. Return to work depends on the type of work and whether driving is necessary. Swimming is encouraged once the sling is of. Overhead and Contact sports are to be avoided for 4 months.
What happens to Rotator cuff tendon tears if they are not repaired?
Unfortunately, the rotator cuff tendons do not heal. If they are left without treatment, the pain may or may not get worse but the tendon tear will tend to get bigger in time. Occasionally, the tear, over a period of years, becomes so big that it can't be repaired.
Also, the muscle attached to the torn tendon tends to change to fat, as it is unable to function. This process occurs very slowly over a period of years but is not reversible even if the tendon is repaired.
Back to top